 If you suffer from insomnia or if you do not awaken refreshed each morning ready to face the day, you need to pay attention to this.
If you suffer from insomnia or if you do not awaken refreshed each morning ready to face the day, you need to pay attention to this.
According to the National Institutes of Health, sleep deficiency is a broad concept that occurs (a) if an individual does not get enough sleep (sleep deprivation), (b) if an individual’s sleeping habits are out of sync with the body’s natural circadian rhythm (sleeping during the wrong time of the day), and (c) if the quality or quantity of sleep is diminished due to a sleep disorder or external factors.
In a 2013 study, the National Sleep Foundation reported that less than half of all Americans (44%) and Canadians (49%) receive a good night’s sleep almost every night. This is a significant health issue.
Adequate Sleep is Important
Sleep is essential to human health. According to a study published in 2005 (Ref. 1) sleep deprivation results in the potential for cell injury and disease due primarily to the resulting reduction in antioxidant levels, particularly glutathione.
Catalase activity and glutathione content, which normally are tightly regulated, were both decreased in liver by 23–36% by 5 and 10 days of sleep deprivation. Such levels are associated with impaired health in other animal models of oxidative stress-associated disease. The decreases were accompanied by markers of generalized cell injury and absence of responses by the other enzymatic antioxidants under study. Enzymatic activities in the heart indicated an increased rate of oxidative pentose phosphate pathway activity during sleep deprivation.
Lack of sleep could increase risk factors for heart disease. According to a 2015 study (Ref. 2):
Decreased quantity and quality of sleep, whether due to sleep disorders or just through lack of proper sleep patterns, have been linked to cardiovascular disease (CVD) risk factors, such as hypertension, obesity, diabetes, and dyslipidemia. Studies have shown that short durations of sleep are associated with greater risk of developing or dying from CVD.
Furthermore, REM (Rapid Eye Movement) sleep is essential to memory and cognitive function. According to a study published in 2009 (Ref. 3):
Compared with quiet rest and non-REM sleep, REM enhanced the formation of associative networks and the integration of unassociated information. Furthermore, these REM sleep benefits were not the result of an improved memory for the primed items. This study shows that compared with quiet rest and non-REM sleep, REM enhances the integration of unassociated information for creative problem solving.
As a side note, intentional sleep deprivation is used as an interrogation technique by police and military forces around the world to take advantage of this phenomenon. There is evidence to suggest that sleep deprivation can lead to false confessions.
REM sleep, however, only occurs during longer periods of deep sleep. It is also during REM sleep cycles that many of the body’s self repair functions are undertaken. People who experience REM sleep tend to dream; but perhaps more importantly, they tend to wake up refreshed and energetic.
What Can You Do?
I would offer four concrete suggestions to improve your sleep situation: avoid stimulants late in the day, schedule your sleep, increase your glutathione levels and get rid of blue light at bed time. Let’s take a look at each of these.
Avoid Stimulants
This is rather obvious but needs to be stated. Many people are in the habit of having coffee or tea after their evening meal. Nicotine (e.g., from smoking) is also a stimulant. But if there is a stimulant like caffeine floating around in their blood stream when it’s time to go to bed, people are unlikely to feel the need to go to bed; when they do go to bed, they are unlikely to go to sleep quickly; and their sleep may not be as restful as it needs to be.
Recommendation: Avoid consuming stimulants in any form for at least eight hours before bed time.
Schedule Sleep
I like to read and do so often in the evening. I guess I inherited that from my dad. He would read Westerns by authors like Zane Grey and Louis L’Amour until all hours. When he was reading he was totally absorbed in the book. Mom used to say she could announce the outbreak of World War Three and he would be oblivious.
I’m the same way. But my preferred genre for escaping reality is sappy romances. (Please don’t tell anyone. It would destroy my macho image.) There have been times when reading late at night that pressure on my bladder forced me to become aware of my surroundings again – and I would realize it was two in the morning. I have had to set the alarm on my mobile phone to remind me to go to bed.
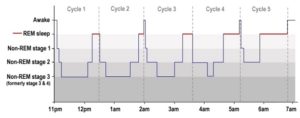 When planning the amount of sleep you need, remember that the beneficial effects of sleep occur during REM sleep cycles. The first cycle lasts about 90 minutes while later cycles last 100-120 minutes. Optimally you should experience five cycles for a good night’s sleep. This forms the scientific basis for the common recommendation that you need 7-8 hours sleep each night.
When planning the amount of sleep you need, remember that the beneficial effects of sleep occur during REM sleep cycles. The first cycle lasts about 90 minutes while later cycles last 100-120 minutes. Optimally you should experience five cycles for a good night’s sleep. This forms the scientific basis for the common recommendation that you need 7-8 hours sleep each night.
Recommendation: Determine when you need to get up the next day. Then figure out when you need to get to bed in order to have the time to get an adequate amount of sleep. Then set an alarm for that time so that you actually have a chance of getting your needed sleep.
Remember: An inadequate amount of sleep constitutes sleep deprivation and that is bad for you.
Increase Glutathione Levels
Studies have shown that people with primary insomnia have low levels of glutathione in their bodies. (Ref. 4) If you have low levels of glutathione in your body there is a high probability that, even if you don’t suffer insomnia, you may not experience restful sleep. People with normal levels of glutathione tend to experience REM sleep cycles and awaken refreshed. From about age 20, the body’s natural glutathione production drops by 1 to 1.5% annually. Other environmental factors further diminish the level of available glutathione in most people. Therefore it is not surprising that so many report inadequate sleep patterns.
Recommendation: One important way to counter this situation is to increase your body’s intracellular glutathione levels.
Avoid Blue Light
As I mentioned, I like to read late in the evening to relax. I used to read physical books. But in the past few years I have taken to reading e-books on my laptop or on my phone instead. Coincidentally I have quite frequently found myself reading well into the early hours of the morning without feeling sleepy. This was disastrous when I had morning business meetings. Having my morning alarm sound after only a couple of hours sleep was not pleasant.
I have had reason to monitor my blood pressure more diligently over the last few months (following a cardiac event). My blood pressure tended to stay in a good range. But I noticed a blood pressure increase later in the day on many days. I worked with some professionals to try to get a handle on what was going on but the results of our analysis have so far been inconclusive. During the course of this, one of the health professionals that was helping with this analysis mentioned that there is a correlation of sleep deprivation to higher blood pressure.
Serendipity. I came across an article that shed some light on the issue (no pun intended). The following is an extract from an article entitled Sleep Disorders by Lisa Marshall in the July/August 2016 issue of Discover Magazine.
As recently as the 1980s, researchers assumed the human sleep-wake cycle was not sensitive to light, recalls Charles Czeisler, chief of the sleep and circadian disorders division at Brigham and Women’s Hospital. “In reality it is the most important synchronizer of human circadian rhythms.” In the 80s, Czeisler discovered that specialized ganglion cells in the retina are finely tuned to tell the brain to cut melatonin production when they are hit by a short wavelength, (around 480 nanometers) – precisely that of morning light. Unfortunately, most phone and tablet screens and LEDs emit a similar bluish wavelength, making them exponentially more potent than older yellowish-orange incandescent bulbs. One 2014 study found sleep lab subjects who read from an iPad before bed say nighttime melatonin levels plummet 55 percent after five days (paper book readers saw no reduction). They also took longer to fall asleep, had less REM-stage sleep and were groggy in the morning.
 This mirrored my experience pretty closely. So what could I do?
This mirrored my experience pretty closely. So what could I do?
I discovered that my laptop and my phone had a setting that would remove this blue spectrum from the display for selected time periods. I turned this setting on and then proceeded to follow my normal reading patterns. What I discovered was that I would get sleepy while reading on my laptop well before midnight (a change from the past several years). And when I went to bed I was able to get to sleep much more quickly and my sleep was more rejuvenating.
Recommendation: Go to the display settings for your electronic devices and set the Night Shift setting to go on at sunset and off at sunrise.
Summary
I’m starting to sleep pretty well.
- I haven’t had coffee on a regular basis for several years and I don’t smoke. So I have managed to avoid stimulants before bed.
- I have my alarm set on my phone to remind me when it’s time to go to bed.
- I take a nutritional supplement that allows my body to produce glutathione on demand so my glutathione levels are much higher than would be expected for someone my age.
- And finally I avoid exposure to the troublesome blue spectrum light from my electronic devices in the hours leading to bed time.
Let me know what your experience has been.
References:
Reference 1: Carol A. Everson, Christa D. Laatsch, and Neil Hogg, Antioxidant defense responses to sleep loss and sleep recovery, American Journal of Physiology – Regulatory, Integrative and Comparative Physiology, Published 1 February 2005 Vol. 288 no. 2, R374-R383 DOI: 10.1152/ajpregu.00565.2004
Reference 2: Michelle Kohansieh and Amgad N. Makaryus, Sleep Deficiency and Deprivation Leading to Cardiovascular Disease, Published May 2015, International Journal of Hypertension, Volume 2015 (2015), Article ID 615681
Reference 3: Denise J. Cai, Sarnoff A. Mednick, Elizabeth M. Harrison, Jennifer C. Kanady and Sara C. Mednick, REM, not incubation, improves creativity by priming associative networks, Proceedings of the National Academy of Sciences of the United States of America, Published 23 June 2009, vol. 106 no. 25 10130-10134, 10.1073/pnas.0900271106
Reference 4: Mustafa Guleca, Halil Ozkolb, Yavuz Selvic, Yasin Tuluceb, Adem Aydinc, Lutfullah Besirogluc, Pınar Guzel Ozdemirc, Oxidative stress in patients with primary insomnia, Progress in Neuro-Psychopharmacology and Biological Psychiatry, Volume 37, Issue 2, 1 June 2012, Pages 247–251
#sleep #glutathione #health
 This is a topic that is somewhat dear to my heart. My sister was diagnosed with Fibromyalgia a couple of decades ago. And her life has been miserable for much of that time.
This is a topic that is somewhat dear to my heart. My sister was diagnosed with Fibromyalgia a couple of decades ago. And her life has been miserable for much of that time. Post Traumatic Stress Disorder (PTSD) has probably been around for thousands of years. But it is only in the last hundred years or so that it has been recognized as a distinct psychological disorder. Its prevalence first came to public awareness during World War I. Front line soldiers in the trenches of Europe, who were the target of massive artillery barrages, were under constant stress, never knowing whether the next artillery round or bullet had their name on it. And this went on sporadically over several years.
Post Traumatic Stress Disorder (PTSD) has probably been around for thousands of years. But it is only in the last hundred years or so that it has been recognized as a distinct psychological disorder. Its prevalence first came to public awareness during World War I. Front line soldiers in the trenches of Europe, who were the target of massive artillery barrages, were under constant stress, never knowing whether the next artillery round or bullet had their name on it. And this went on sporadically over several years. Symptoms can include:
Symptoms can include: A few years ago my daughters started expressing concern for my health. They nagged and cajoled at every opportunity, telling me I needed to get in better shape. I knew they were right but I didn’t want to go to the effort to change. I would huff and puff going up a flight of stairs. I admit that I was a little overweight. (Alright, I’ll tell the truth. I was obese.) I paid a premium price for most of my clothes because I had to shop in a large men’s specialty clothing store.
A few years ago my daughters started expressing concern for my health. They nagged and cajoled at every opportunity, telling me I needed to get in better shape. I knew they were right but I didn’t want to go to the effort to change. I would huff and puff going up a flight of stairs. I admit that I was a little overweight. (Alright, I’ll tell the truth. I was obese.) I paid a premium price for most of my clothes because I had to shop in a large men’s specialty clothing store.